Some thoughts from a RAMCOA survivor
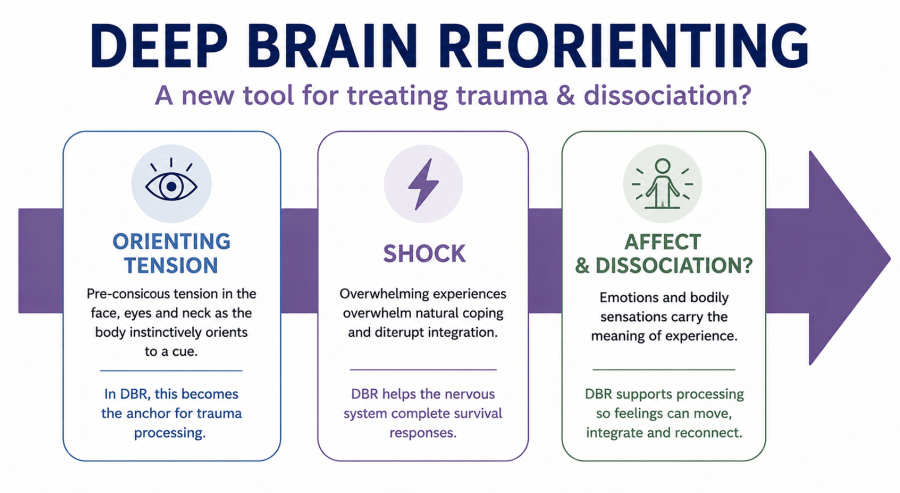
Deep Brain Reorienting (DBR) is a relatively new trauma therapy developed by Frank Corrigan that is gaining attention in the trauma and dissociation field. Unlike therapies centred on narrative reconstruction or emotional catharsis, DBR works with what it proposes are the brain’s earliest survival responses: the orienting and shock reactions that occur milliseconds before conscious emotional overwhelm.
For survivors of severe developmental trauma and dissociation, this feels significant.
Many of us do not primarily hold trauma as a coherent story. Trauma may be encoded through body states, autonomic reactions, fragmented imagery, sensory impressions, and dissociated conditioned survival responses. That is often why conventional talk therapy feels so limited. The body remembers what the mind cannot easily verbalise.
What a DBR session looks like
A DBR session is preferably delivered eyes-closed. It is usually very slow, internally focused, and far less verbally driven than conventional psychotherapy. Rather than recounting trauma in detail, the therapist helps guide attention toward subtle bodily and attentional experiences linked to the earliest stages of activation.
Questions may include:
- What did your body notice first?
- What happened just before the fear?
- What impulse did you notice in your eyes, neck, or head?
- Stay with that sensation.
Attention is often directed toward micro-experiences such as:
- eye movement impulses
- neck or head tension
- changes in body sensation
- shifts in spatial awareness
- autonomic reactions
- shock responses
- impulses to orient toward or away from danger
Clients describe entering a deeply absorbed internal state. Attention narrows. Body awareness intensifies. Internal imagery may become vivid. Time may feel altered. Small nervous system shifts become more noticeable.
Unlike therapies that deliberately intensify emotional activation, DBR slows everything down. That pacing may be especially important for highly dissociative survivors.
The orienting response and why it matters
At the centre of DBR is the orienting response: the nervous system’s automatic reflex toward something novel, threatening, or emotionally important.
This happens before conscious thought. Before fear fully emerges. Before panic, rage, collapse, or dissociation.
The body notices first.
In attachment trauma, especially where caregivers were both the source of safety and danger, these orienting responses may become deeply dysregulated. The nervous system can remain locked in unresolved cycles of vigilance, freeze, shock, or defensive withdrawal.
DBR attempts to access trauma here, before the full cascade of overwhelm begins.
For survivors with DID, that feels highly relevant.
Eyes closed, imagery, and internal focus
One of the most interesting parts of DBR is how closely it relates to visual attention.
The orienting reflex is tied to visual-attentional networks and eye movement systems, including structures such as the superior colliculus. These systems can activate even with eyes closed.
Mental imagery recruits many of the same neural pathways as visual perception. During trauma recall or visualisation, people may notice subtle eye impulses under closed eyelids: scanning, gaze aversion, fluttering, fixation, or urges to look away.
The body may orient toward internally generated threat as though it were physically present.
This strongly complements my own understanding of effective trauma work with RAMCOA and DID.
I suspect the intense inward focus used in DBR may reduce ordinary analytical thinking while increasing access to sensory, emotional, and imagery-based processing systems linked to implicit trauma memory.
That may help explain why some survivors report entering deeply absorbed internal states during DBR.
I also suspect this can resemble a mild trance state. For highly dissociative survivors, that may feel familiar. DBR attempts to keep enough dual awareness present so the nervous system can process without tipping fully into dissociation.
DBR and EMDR
DBR shares some similarities with EMDR.
Both involve focused attention. Both activate traumatic material while keeping some awareness anchored in the present. Both engage implicit trauma networks rather than relying purely on verbal cognition.
A difference seems to be timing.
EMDR often activates more formed memories and emotions relatively early and uses bilateral stimulation to assist processing.
DBR appears to work earlier in the sequence, at the level of orienting, shock, and autonomic activation before full emotional response emerges.
It is slower and more tightly titrated.
For highly dissociative clients, that pacing may reduce flooding and make the work feel more tolerable.
The window of tolerance and Sebern Fisher’s neurofeedback
A major challenge for severe dissociative survivors is remaining within Daniel Siegel’s “window of tolerance.”
DBR therapists aim to keep clients regulated enough to stay present without becoming overwhelmed, collapsing, or dissociating.
But survivors of extreme abuse may automatically shift into internally absorbed or dissociative states because that was learned very early as a survival strategy either naturally or via forced conditioning.
This is where Sebern Fisher’s work with neurofeedback feels relevant.
Her work on developmental trauma emphasises that before many dissociative clients can safely process trauma, the nervous system may first need help building regulation and flexibility.
Dissociation, hypervigilance, emotional flooding, chronic shutdown and fragmentation are not simply psychological symptoms. They often reflect longstanding nervous system dysregulation.
From that perspective, neurofeedback may help strengthen regulation, improve access to present-day awareness, and expand the capacity to stay with difficult material without immediately leaving the body or fragmenting.
For many survivors, that regulation may be the foundation that makes deeper trauma processing possible.
Hypnosis as preparation
I also suspect carefully structured hypnotic techniques may complement DBR well.
In this context, hypnosis is not about suggestion or control. It is about attentional regulation, nervous system calming, and maintaining stability within altered internal states.
This may help with:
- controlled attentional narrowing
- strengthening dual awareness
- grounding during internally absorbed states
- increasing affect tolerance
- reducing panic during inward focus
- improving physiological relaxation
- tolerating traumatic imagery without immediate dissociation
Progressive relaxation, slowed breathing, visualisation, counting, or guided descent imagery may all help reduce cognitive resistance and support entry into a more regulated internally focused state.
Many dissociative survivors already have unusually strong capacities for absorption and imagery. In my view, hypnosis can help stabilise states that are already neurologically familiar.
Combined thoughtfully, neurofeedback may help regulate the system beforehand, hypnosis may help focus and stabilise attention, and DBR may help access the orienting and shock responses held underneath conscious memory.
That combination feels clinically meaningful.
Why this may matter for DID
DID often develops in the context of impossible attachment conflict.
A child must move toward the caregiver for survival while simultaneously fearing that same caregiver as a source of danger.
That conflict creates profound disorganised attachment.
Over time, overwhelming bodily, emotional, and relational experiences may become compartmentalised into dissociated self-states because they could not be integrated developmentally.
DBR may be especially relevant because it attempts to access those deeply encoded survival responses before full defensive activation occurs.
For trauma held primarily in body memory, autonomic states, symbolic imagery, or dissociated fragments rather than narrative recall, this may offer another useful entry point.
Final thoughts
Trauma theory continues shifting toward a deeper understanding of trauma as a disorder of nervous system organisation involving attachment, orienting, autonomic regulation, dissociation, sensory processing, and implicit survival responses.
While DBR is still emerging and further research is needed, I think it may prove to be a valuable addition to the trauma and dissociation toolbox.
For complex trauma and DID, healing is often layered and highly individual. Trauma is stored through a unique combination of sensory experience, body memory, attachment patterns, and survival responses. Therefore, different nervous systems, and separate trauma events, require different pathways to be activated in each therapy session.
In my own work and lived experience, I have found value in combining multiple approaches including neurofeedback, art therapy, Clay Field Therapy, EMDR, Brainspotting, equine therapy, bilateral music, and hypnosis techniques.
Each can approach trauma from a different entry point:
- nervous system regulation
- body memory
- imagery
- sensory processing
- emotional regulation
- attachment repair
Used together, these approaches may support gradual integration of dissociated parts and help resolve deeply embedded attachment trauma.
DBR may offer another pathway into this work by accessing trauma at the earliest level of orienting and survival activation.
For survivors whose trauma sits beneath words and outside ordinary autobiographical memory, DBR may prove especially valuable.
The more therapeutic tools available, the greater the chance of finding an approach that can safely access and help reprocess what has been held for so long. I expect DBR may become one more effective addition to the evolving trauma recovery toolbox.
References
Fisher, S. F. (2025). Neurofeedback in the treatment of developmental trauma: Calming the fear-driven brain (10th anniversary ed.). W. W. Norton & Company.
Kearney, B. E., Corrigan, F. M., Frewen, P. A., Nevill, S., Harricharan, S., Andrews, K., Jetly, R., McKinnon, M. C., & Lanius, R. A. (2023). A randomized controlled trial of Deep Brain Reorienting: A neuroscientifically guided treatment for PTSD. European Journal of Psychotraumatology, 14(2), 2240691.


You must be logged in to post a comment.